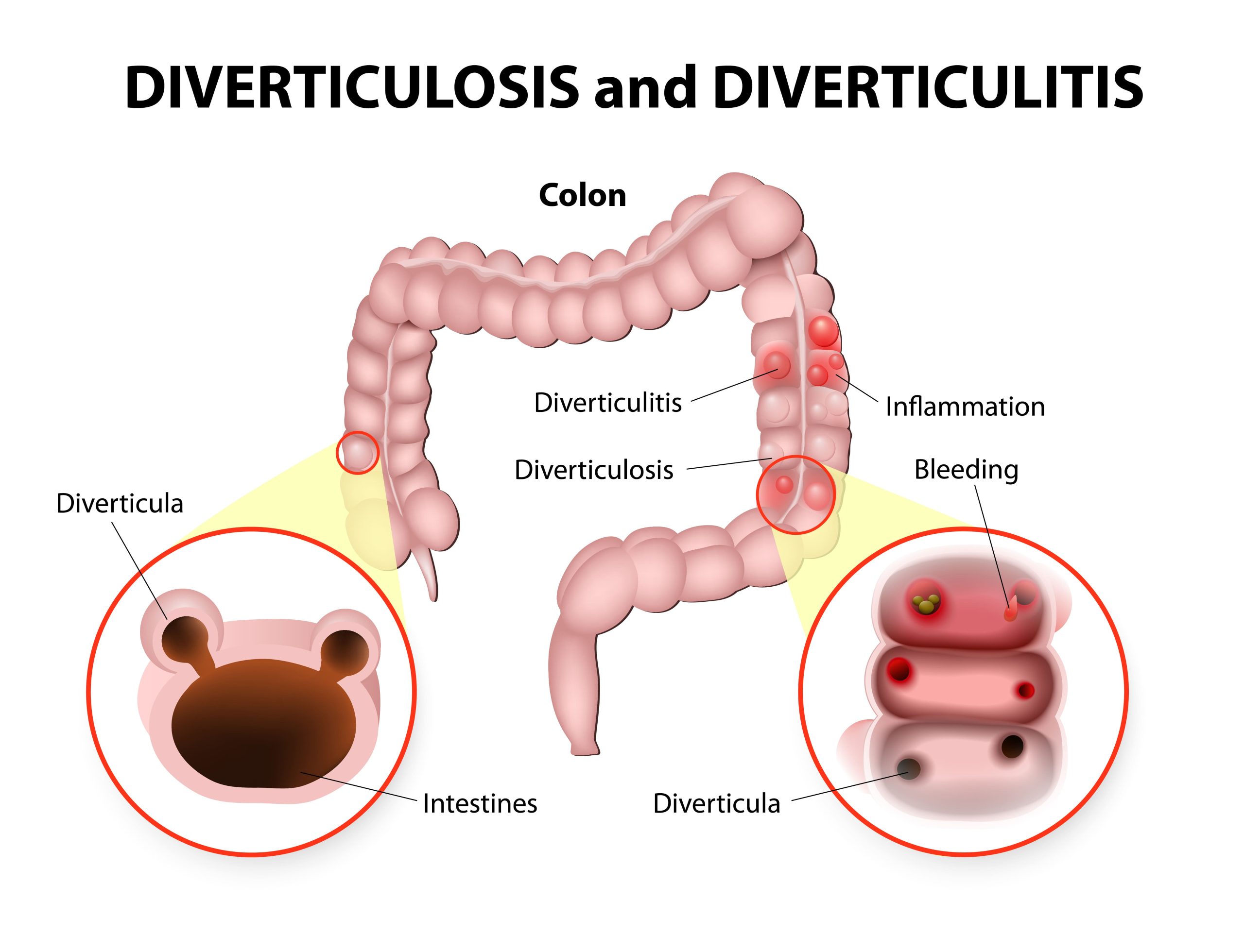
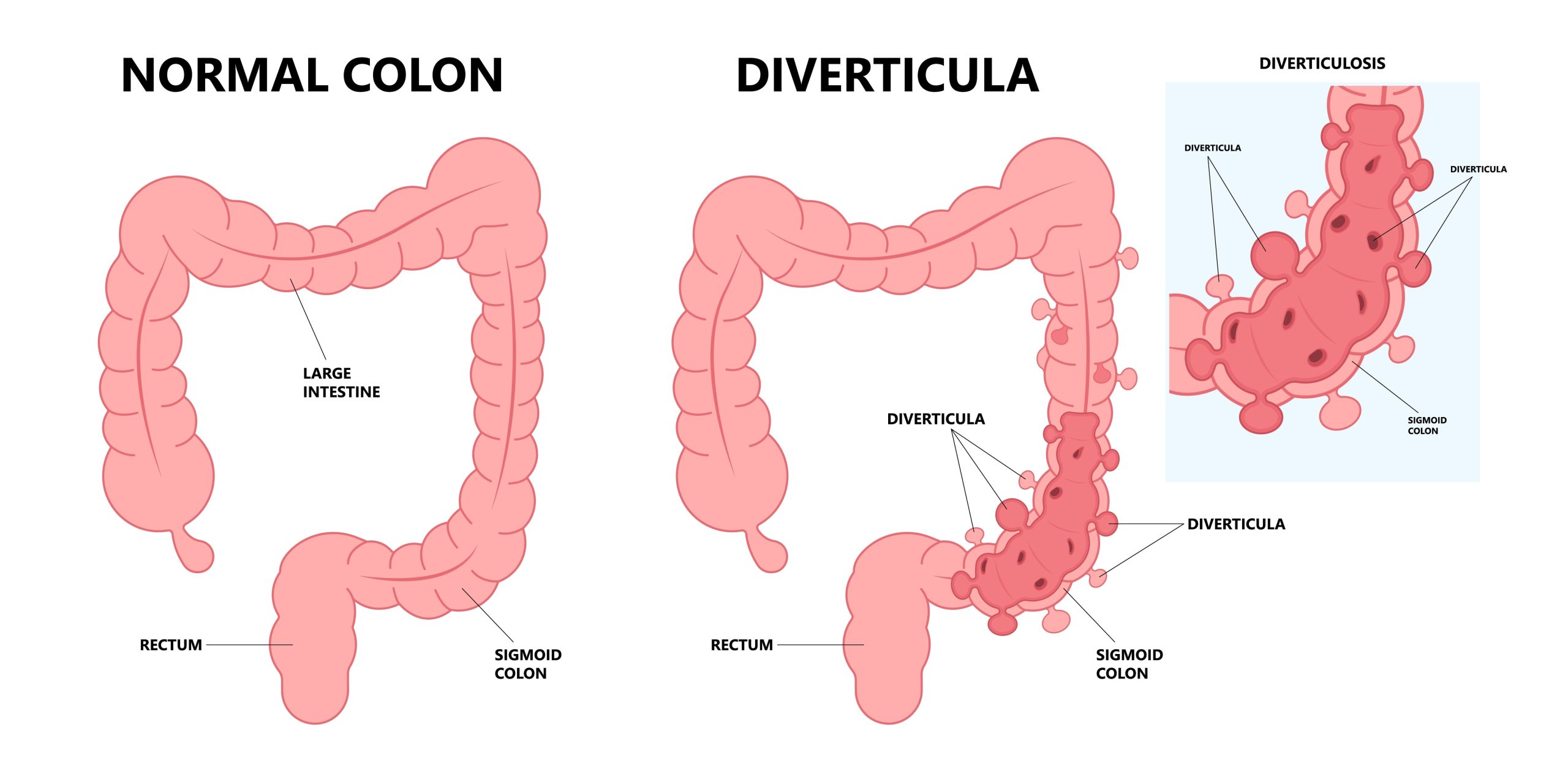
Background of diverticular disease Diverticulosis and Diverticulitis Type Clinical features Definitions Diverticulum Protrusion of colonic wall that forms a sac Abnormal colonic motility exaggerates segmental contractions Increase in intraluminal pressure leads to herniation of mucosa and submucosa Diverticulosis Up to 45% prevalence in Western countries Presence of many diverticula that can be asymptomatic or symptomatic Most commonly in sigmoid colon Easily visualized on colonoscopy Diverticular disease Clinically significant and symptomatic diverticulosis Diverticular bleeding Painless blood in stool Herniation of diverticulum leads to injury of surrounding vasa recta Artery weakens and ruptures into lumen Diverticulitis Occurs in approximately 4-15% of patients with diverticulosis Inflammation of diverticulum that can be acute/chronic and uncomplicated/complicated Erosion of diverticular wall due to increased intraluminal pressure Eventual inflammation, necrosis, and micro/macro perforation Complicated Diverticular abscess Fistula Bowel obstruction Free perforation Segmental colitis Inflammation of mucosa between diverticulum without involvement of the diverticular orifice Unclear pathogenesis but possible mucosal prolapse, fecal stasis, or localized ischemia Symptomatic uncomplicated diverticular disease (SUDD) Persistent abdominal pain without macroscopically visible colitis or diverticulitis Colonic wall thickening without other inflammatory changes on CT imaging Possibly due to abnormal colonic motility or visceral hypersensitivity Risk factors Decreased physical activity Obesity Smoking Dietary Low fiber High fat High red meat intake Medications Nonsteroidal Anti-inflammatory Drugs (NSAIDs) Steroids Opiates (Next Lesson) Clinical presentation of acute diverticulitis Back to Diverticulosis and Diverticulitis No Comments Comments are closed.
{kind=link}
{kind=link}
{kind=link}
No Comments