| Type | Clinical features |
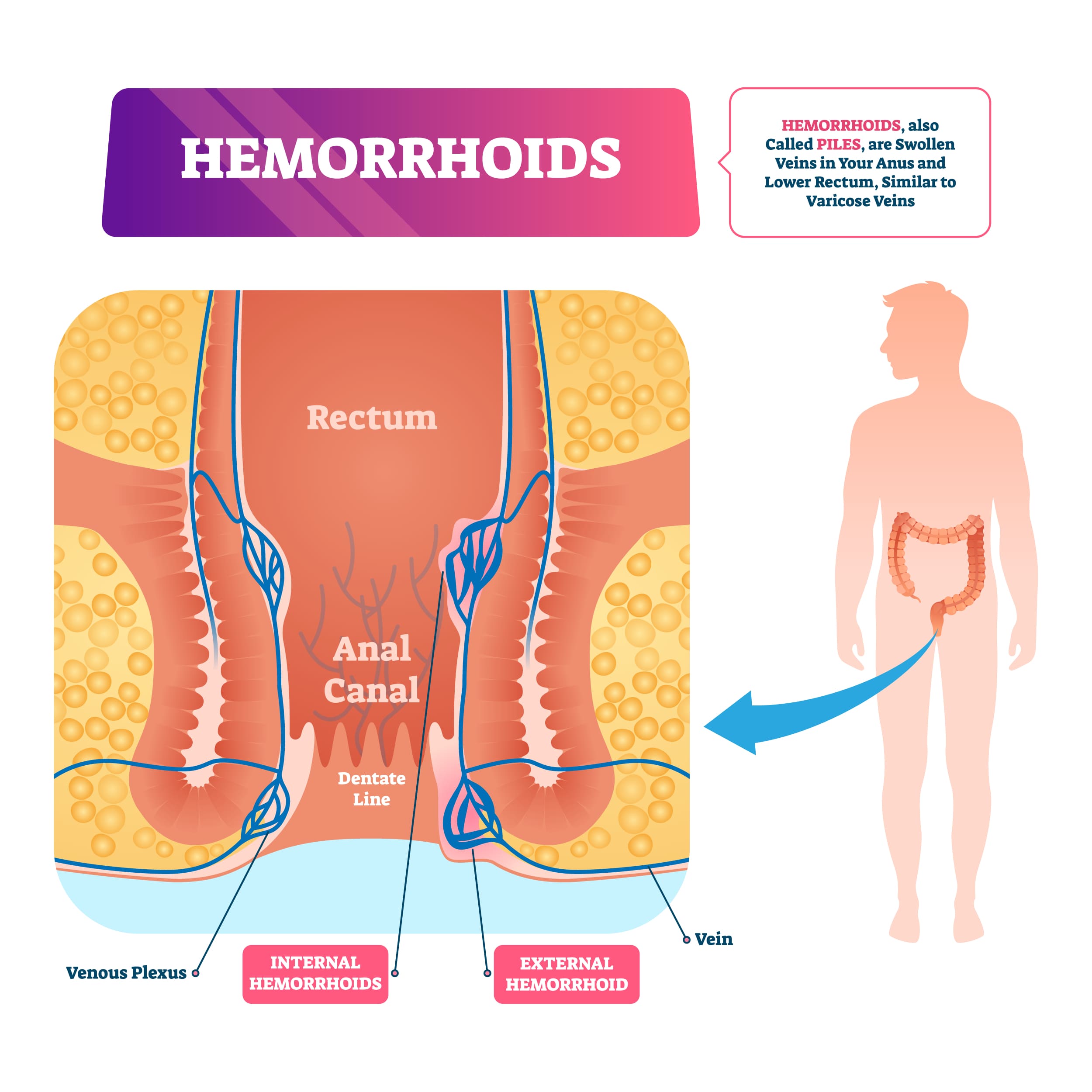
| Definitions | - Normal vascular structures from channel of arteriovenous connective tissues draining into superior and inferior hemorrhoidal veins
- Located distal to anal dentate line
- Arise from inferior hemorrhoidal plexus and covered by modified squamous epithelium with pain receptors
- Located proximal to anal dentate line
- Arise from superior hemorrhoidal plexus and can occur in left lateral, right anterior, or right posterior regions
- Covered by columnar epithelium without pain receptors
- Located both proximal and distal to anal dentate line
|
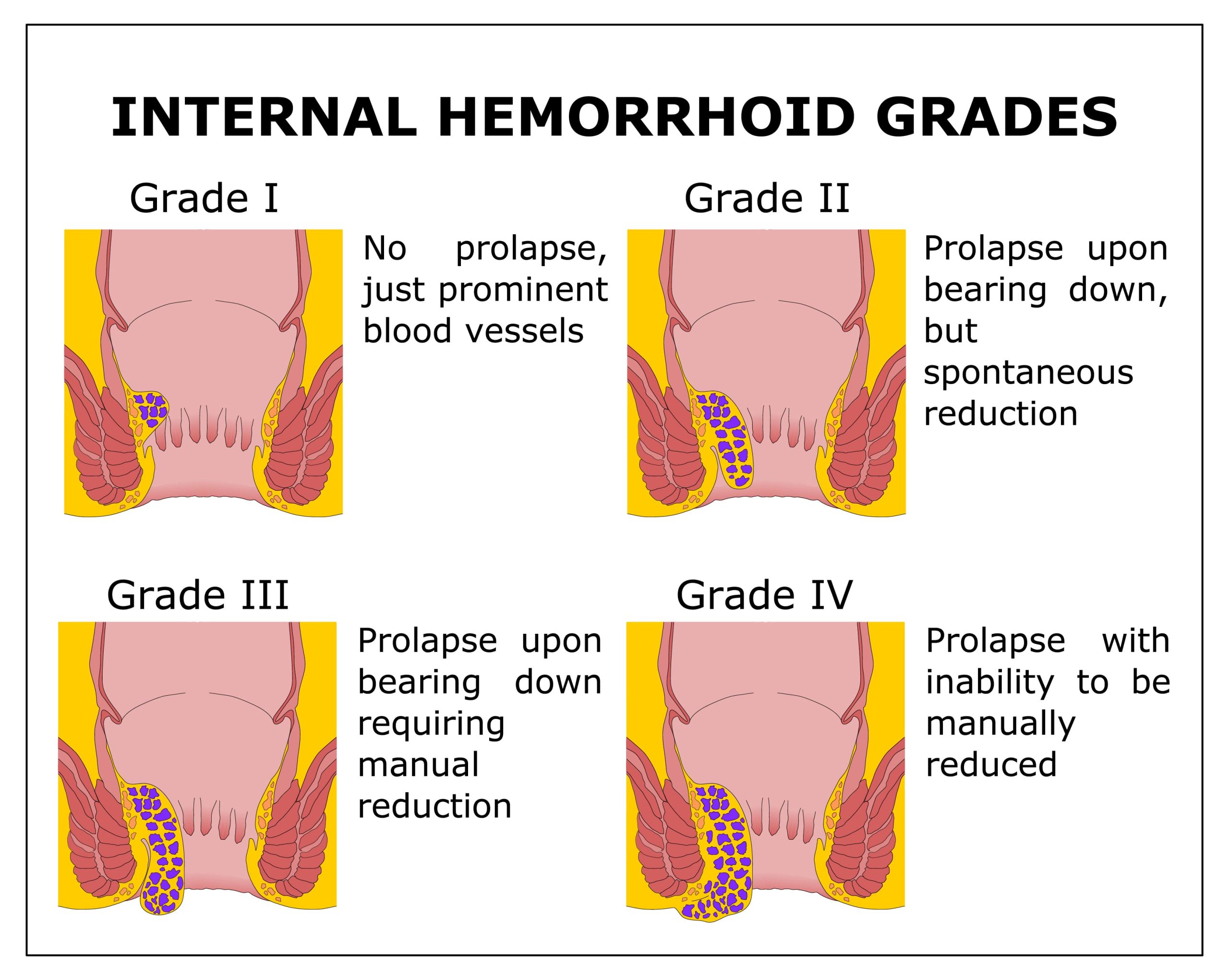
| Classification of internal hemorrhoids | - Can bulge into lumen without prolapsing below dentate line
- Prolapse out of anal canal with defection or straining
- Spontaneously go back into anal canal
- Prolapse out of anal canal with defection or straining
- Requires manual reduction
- Prolapse out of anal canal continuously
- Cannot be reduced and may strangulate
|
| Possible Pathogenesis of hemorrhoids | - Deterioration of connective tissue anchoring hemorrhoids, which causes them to slide into anal canal
- Increased anal sphincter tone forcing hemorrhoidal plexus against internal sphincter
- Abnormal distention of arteriovenous anastomoses within the hemorrhoidal plexus
- Abnormal dilation of veins in hemorrhoidal plexus
|
| Possible risk factors | - Anticoagulation or antiplatelet therapy
|
{kind=link}
{kind=link}
No Comments